Testosterone Therapy and Fertility: What Men Actually Need to Know About Long-Term Use
For men 30–50 juggling work, family, and health; who want straight answers about TRT, protecting fertility, and whether ‘once you start, you can’t stop’ is really true.
If you’re researching testosterone replacement therapy, you’ve probably encountered two extremes: clinics promising life-changing results, and online forums warning that TRT means lifelong dependency and destroyed fertility.
The truth is more nuanced and more reassuring than either narrative suggests.
This guide is for men who want to understand how testosterone therapy actually works, what creates real risk versus unnecessary fear, and how to protect both your current quality of life and your future health.
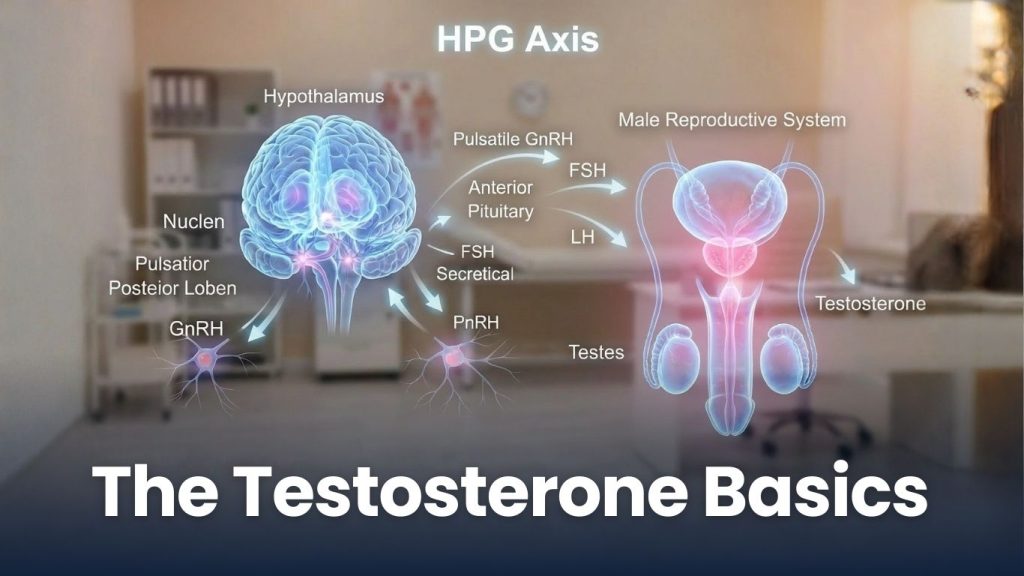
Testosterone Basics
Your body produces testosterone through a carefully regulated system called the hypothalamic-pituitary-gonadal (HPG) axis. Here’s how it works:
The normal cycle:
- Your hypothalamus (in the brain) releases GnRH
- Your pituitary gland responds by releasing LH and FSH
- These hormones signal your testes to produce testosterone and sperm
- When testosterone rises, your brain detects this and reduces the signal
This feedback loop is how your body maintains hormonal balance naturally. It’s not fragile, it’s adaptive.
Why this matters for treatment: Understanding this system explains why different testosterone therapies affect fertility differently, and why “dependency” isn’t about the testosterone itself; it’s about how treatment interacts with this natural cycle.

Will TRT Make You Dependent?
Let’s address the biggest concern directly: Will starting testosterone therapy mean I can never stop?
What dependency actually means:
- Prolonged suppression of natural production without monitoring or adjustment
- Stopping therapy abruptly after years of use, leading to temporarily low levels during recovery
- Treatment models that never reassess dosing, alternatives, or whether therapy is still needed
What dependency does NOT mean:
- Permanent, irreversible loss of natural testosterone production
- A lifetime commitment after one injection
- Automatic fertility destruction
- Loss of all treatment options except continuing current therapy
The critical distinction: Dependency is usually a result of poor treatment design, not an inherent property of testosterone therapy itself.

Testosterone Therapy and Fertility: Separating Fact from Fear
The real mechanism: Sperm production requires two things: FSH signaling from the pituitary, and adequate intratesticular testosterone (testosterone levels inside the testes, distinct from blood levels).
Some testosterone treatments can reduce FSH and intratesticular testosterone. This reduction in the FSH is an effect that is not always final, often reversible, and preventable with the right protocols.
Fertility outcomes depend on which treatment approach is used and how it’s monitored. Not on whether you’re addressing low testosterone at all.
Many men maintain or preserve fertility while treating their low testosterone symptoms. Though it requires intentional planning, not lucky genetics.
Comparing Testosterone Treatment Options: TRT, Enclomiphene, and HCG
Different approaches affect the HPG axis differently.
Traditional Testosterone Replacement Therapy (TRT)
How it works: Provides testosterone directly (injections, gels, or pellets) to raise blood levels.
Effect: Can suppress LH and FSH over time, potentially reducing sperm production if used alone.
Best for: Men with clearly low testosterone who are not currently trying to conceive, or who are using fertility preservation strategies.
Fertility consideration: Often paired with HCG or other medications to maintain testicular function and sperm production.
Enclomiphene (Selective Estrogen Receptor Modulator)
How it works: Stimulates your brain to increase LH and FSH, encouraging your body to produce its own testosterone.
HPG axis effect: Maintains or enhances natural signaling, typically preserves sperm production.
Best for: Men concerned about fertility, or those who prefer stimulating natural production over direct replacement.
Consideration: Testosterone increases are generally more moderate than with TRT. Not the solution for all causes of low testosterone.
HCG (Human Chorionic Gonadotropin)
How it works: Mimics LH, directly signaling the testes to produce testosterone.
HPG axis effect: Maintains intratesticular testosterone and can preserve fertility even alongside TRT.
Best for: Men who want symptom relief and active fertility preservation, or those using TRT who want to maintain testicular function.
Consideration: Requires careful dosing and monitoring. Often used in combination protocols.

What Responsible Testosterone Therapy Actually Looks Like
Quality care isn’t about promising perfect outcomes. It’s about measurement, adjustment, and protecting long-term options.
Essential elements of good TRT care:
Comprehensive baseline testing:
- Total and free testosterone
- Estradiol
- Complete blood count (hematocrit monitoring)
- Metabolic markers
Fertility assessment when relevant:
- Semen analysis before starting treatment
- Discussion of family planning timeline
- Proactive fertility preservation strategies
Ongoing monitoring:
- Regular lab work (typically every 3-6 months)
- Dosing adjustments based on response
- Periodic evaluation with licensed providers on treatment
Treatment flexibility:
- Willingness to adjust approach based on changing goals
- Options for fertility preservation or restoration
- Clear protocols for discontinuation if desired
Red flags to watch for:
- Clinics that prescribe without comprehensive labs
- One-size-fits-all dosing protocols
- Dismissal of fertility concerns
- No discussion of monitoring or future flexibility
- Pressure to commit without questions
Let’s talk about the “Clinic Revenue Model”
This skepticism is legitimate. Some clinics prioritize patient retention over patient outcomes.
How to identify patient-centered care:
- They discuss alternatives: Including non-testosterone options like lifestyle optimization, sleep improvement, or addressing underlying causes
- They plan for fertility: Proactively, not as an afterthought when you ask.
- They adjust dosing down: When appropriate and not just up.
- They talk about stopping: Including what restoration of natural production looks like, and when it might make sense.
- They order comprehensive labs: Not just total testosterone.
- They explain trade-offs honestly: Responsible clinicians put their patients needs before their own. If a treatment isn’t right, they won’t advise it.

Why Taking Testosterone Seriously Isn’t a Sign of Weakness
Modern hormone care isn’t about chasing numbers on a lab report or committing to a rigid protocol for life. It’s about understanding how your hormones support the life you’re building over the long term. That’s your energy, focus, fertility, and ability to show up consistently. Approaches like HCG therapy or enclomiphene can help preserve reproductive function when used appropriately, but the deeper shift is recognizing health as something to manage proactively, not something to address once it’s already compromised. Letting go of outdated stigma around testosterone therapy allows men to make informed, deliberate decisions about their wellbeing. Being proactive about your testosterone doesn’t make you weak. You reflect responsibility in your health. The same responsibility that you apply to your career, your health, and your family’s future.
You Have More Options Than You Think
If you start TRT, you’re not trapped. Treatments can be discontinued, protocols can be adjusted, and your goals can change! If your goals change, your treatment does too. A protocol that makes sense at 35 (not planning children) might shift at 38 (family planning active) and evolve again at 45. Quality care is adjustable to you and what you need.

Key Questions for Your Doctor
Before starting any testosterone therapy here are some questions you can ask the licensed providers:
- “What are the specific causes of my low testosterone?”
- “How will this treatment affect my fertility, and what preservation options do you recommend?”
- “What monitoring will happen, and how often will we reassess whether this approach is still right?”
- “What does stopping or transitioning to a different approach look like?”
- “How do you dose testosterone and do you ever reduce doses or discontinue therapy?”
- “What happens if my life circumstances change (wanting children, moving, changing insurance, etc.)?”
The quality of their answers matter more than which specific treatment is suggested.
The Bottom Line: Informed Decisions are Key
Testosterone therapy is neither a reckless commitment nor a magic solution. It’s a medical intervention that, when done thoughtfully, can significantly improve quality of life while protecting long-term health and fertility.
The real risks aren’t from testosterone itself.
You’re not choosing between “natural” and “dependent.” You’re choosing between thoughtful medical care that protects your options, and rigid protocols that don’t. That’s a choice worth making carefully.
Next Steps
If you’re considering testosterone therapy:
- Get comprehensive lab work (not just total testosterone)
- Identify clinicians who discuss fertility proactively
- Ask about monitoring protocols and long-term flexibility
- Consider your family planning timeline
- Understand that starting doesn’t mean permanent commitment
The goal is for you to feel informed and confident that you’re protecting both your current wellbeing and your future options.
This article is for educational purposes and does not constitute medical advice. Testosterone therapy should only be pursued under the guidance of a qualified healthcare provider who can assess your individual situation, monitor treatment appropriately, and adjust protocols based on your evolving health goals.